Appointment slot issues within the NHS e-Referral Service (managing and minimising)
This guidance explains what NHS e-Referral Service appointment slot issues are, the best practice for managing them, and strategies for avoiding them in future.
The NHS e-Referral Service (e-RS) combines electronic booking with a choice of place, date and time for first hospital or clinic appointments. Where offered by the provider, patients can choose their initial hospital or clinic appointment and book it in the GP surgery at the point of referral, or later on the phone or online via the NHS App.
When no clinic appointment is available for patients to book in e-RS, the referral can be forwarded (via the Manage Your Referral patient application/NHS App) or deferred (via the professional application) to the patient’s chosen provider to enable the provider to book the patient an appointment. When a referral is forwarded or deferred, it will appear on that provider’s appointment slot issues (ASI) worklist.
There are 2 reasons why there may be no clinic appointments available on e-RS:
- In very rare circumstances, a technical issue can prevent an appointment slot from being shown or booked.
- The usual reason is that organisations providing directly bookable services have not made sufficient appointment slots available to e-RS.
Problems caused by not managing appointment slot issues effectively
While some appointment slot issues are inevitable, it is important that providers manage them in a timely and effective manner to minimise the effects on patients, referrers and their own staff. The impacts of poor ASI management include:
Best practice to manage and minimise appointment slot issue
Commissioners
Managing demand for a service is a shared responsibility between commissioners and providers. They need to work together to ensure that, where appropriate, a patient is treated at their first choice of provider.
Under the NHS Constitution, commissioners must ensure that patients are able to exercise their legal right to choose which provider they go to for an outpatient appointment with a consultant or specialist.
Commissioners must put the necessary systems in place to ensure patients are offered and supported in their choice and allow patients to book appointments.
Commissioners should work with their local providers to ensure sufficient slots are always made available to allow patients to book their appointments.
Referrers
Referrers should offer the patient a shortlist that includes more than one service or provider in order to minimise the likelihood of the patient encountering an ASI. A letter from NHS England on May 25, 2023 reiterates the need to offer patients a choice of providers:
'We are asking all referrers to ensure they shortlist on average 5 choices from which the patient may choose, where this is practicable, clinically appropriate, and preferred by the patient.'
Referrers need to inform patients that:
- when there are no appointment slots available there is a process within e-RS which enables their appointment request to be passed to their chosen provider who will then contact them to arrange an appointment
- the same process allows them to forward their appointment request to their chosen provider if they try to book online and cannot see any available appointment slots
- where ASIs do occur, they can consider attending any other provider on their shortlist if they wish to do so
- the referrer is able to print a letter to give to the patient or send email to the patient from e-RS explaining what to do next and who to contact if they do not hear from the provider in the designated time (more information on print and email options can be found on the referring a patient page
If a patient contacts their referrer because their chosen provider has not arranged an appointment, this should be escalated to their local commissioner.
Using the defer appointment booking function
When a referrer attempts to book an appointment for a patient and there are no slots available, they can defer the responsibility for booking the appointment to the patient’s chosen provider using the defer appointment booking button.
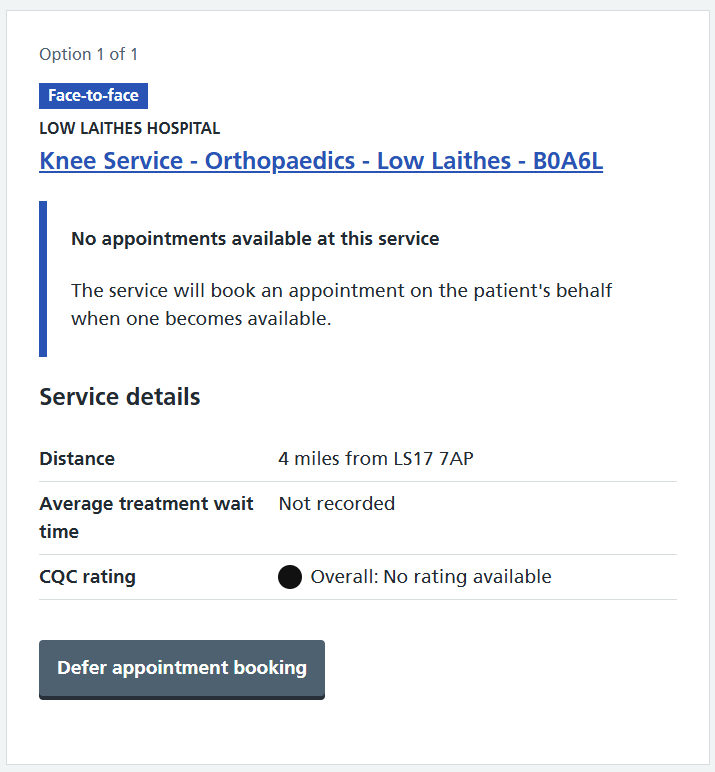
If appointments are available to be booked but are not suitable or convenient for the patient, then the referral cannot be deferred to the provider. Instead, the referrer should discuss alternative providers with the patient. Otherwise the patient will have to wait for suitable appointments to become available.
Once the referrer has selected the defer appointment booking option, the patient must choose which of the services with no slots they would like to be referred to – a referral request can only be deferred to one service. This is done by selecting one of the radio buttons on the deferral options details screen.
From the deferral options summary screen, the referrer can confirm the patient’s choice of provider and print or email (if applicable) the appointment request letter. Both this screen and the letter will indicate a date by when the patient should have heard from their chosen provider and will be based on the priority of the referral.
The date is calculated from the date of deferral plus:
- 2 working days for 2 week wait referrals
- 20 working days for urgent referrals
- 40 working days for routine referrals
The referrer can monitor the status of their patient’s referral via the 'Referrals pending external action' worklist, which will show the referral with a status of 'Deferred to provider' until it is booked.
Patients will not be sent reminders to book appointment while their referral is in a deferred to provider state. This helps to alleviate the frustration experienced by patients who have tried to book an appointment, been told that the provider will contact them and who then receive a letter reminding them to book their appointment.
Providers
Appointment slot issues compound waits by creating a backlog of patients whose waiting time has already started, creates a significant amount of avoidable administrative work and can cause patient safety issues as outlined above.
Providers must remember that:
- they are contractually required to ensure that sufficient appointment slots for first outpatient appointments are available on e-RS as set out in the NHS Standard Contract Service Conditions
- all NHS organisations must have systems in place to promote equality and support all patients in the booking of their outpatient appointments
- they are obliged to accept all clinically appropriate referrals and cannot turn patients away because they are not able to treat them within waiting time targets
- the waiting time clock starts as soon as the referral appears on the provider’s ASI worklist within e-RS
- if the referral is being sent initially through a clinical assessment service (CAS) then the waiting time starts from the date on which the original assessment appointment is booked
- if the referral is sent initially through a referral assessment service (RAS) then the waiting time starts from the date that the clinical referral information is attached to the RAS request, and it then appears on the provider’s referrals for review worklist
Managing the Appointment Slot Issue worklist
Senior managers in provider organisations should ensure that all staff managing the ASI worklists are appropriately trained, are in the correct workgroups and have the necessary skills and authority to manage these referrals effectively and within the required timescales.
If a two week wait referral is entered into the ASI process, it will appear immediately at the top of the provider’s ASI worklist. As outlined above, the patient will expect to be contacted within two working days to arrange their appointment. Providers should make every endeavour to always ensure that there are sufficient appointments available for their two week wait services in order to minimise unnecessary stress to patients. Patients whose two week wait referrals appear on an ASI worklist should be contacted by the provider immediately to have an appointment booked. Urgent and routine patients expect to be contacted within 20 and 40 working days respectively.
The UBRN received date will turn red when the date given to the patient has already passed. Providers must not wait until the UBRN received date turns red on their worklist before they take action as it is likely that the patient will be in the process of contacting either their referrer or service provider to say that they have not received an appointment and potential patient safety issues may be occurring.
If the provider is unlikely to be able to arrange a patient’s appointment within the necessary timescales, the provider should contact the patient to explain the delay and provide details of how they can be contacted with any further queries. The provider should not direct the patient to contact their GP/referrer unless they now wish to book with a service not on their original shortlist.
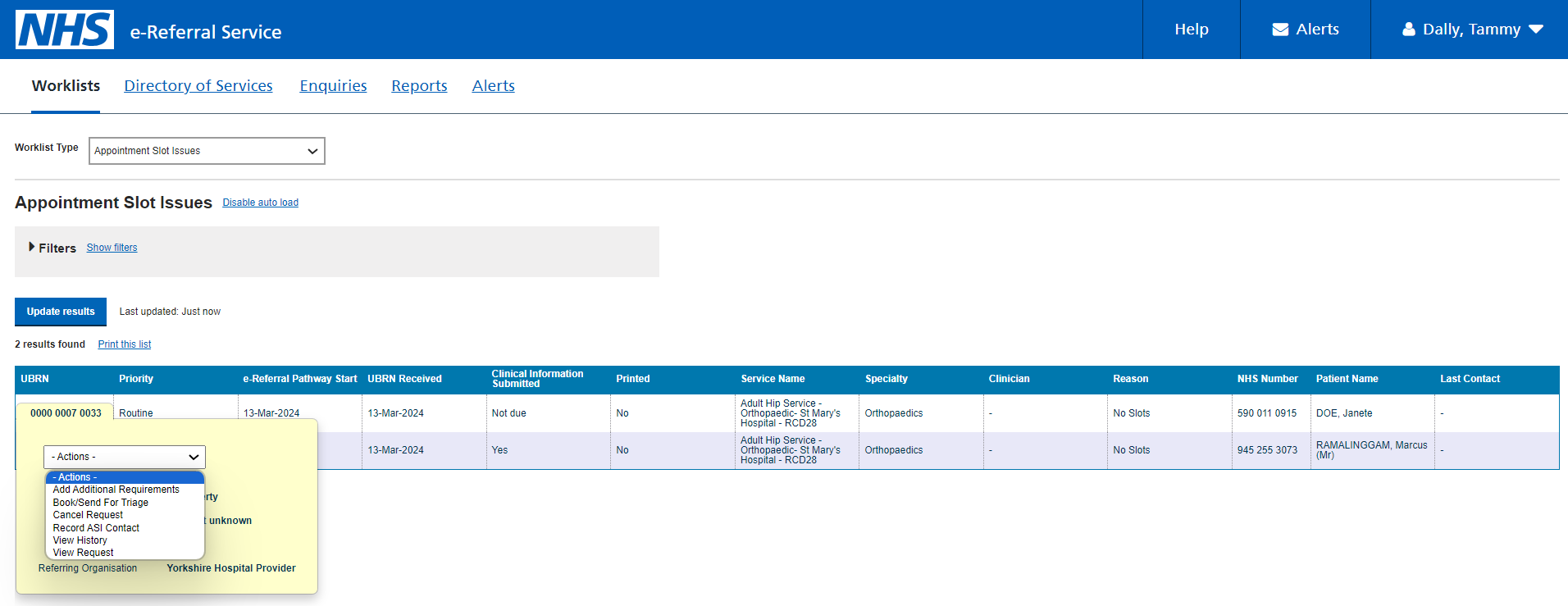
From the ASI worklist providers can perform the following actions:
- add additional requirements
- book appointment
- cancel request
- record ASI contact
- review referral
- view history
- view request
The key actions are further explained below:
Strategies for reducing appointment slot issues
The NHS e-Referral Service programme team has engaged with a several providers who providers to understand how they are implementing strategies to manage outpatient demand and reduce ASIs. There are number of key lessons that can be learned from the processes that these providers have in place which are detailed in the sections below.
The University Hospitals Coventry and Warwickshire have told us about the benefits from reviewing their services:
'Reviewing our capacity linked to e-Referrals for our directly bookable services (DBS) alongside our clinic utilization and booking order has allowed us as a Trust to successful bring patients forward utilising available capacity. This then allowed us to use a patient booking window to ensure capacity is always protected to accommodate any urgent patients and control the capacity patients can see, regaining this control has allowed us to highlight areas of high demand and implement plans to manage this demand before needing to extend the horizons and increase the wait times.
Closing booking for 2024 allowed us to monitor our demand and review our services which were currently DBS and promote the benefits of the services with the highest demand to become a referral assessment service while reviewing the current services offered.'
Appointment slot issues management information
The correct use of data and information contained within the e-RS is fundamental to the management of ASIs by both commissioners and providers. It enables the incidence of ASIs to be calculated, monitored and discussed at national, regional and local levels.
The monthly ASI report enables providers and commissioners to look at ASIs by type and by specialty. Importantly, it helps to compare the number of ASIs with the number of overall bookings, showing this as a ratio. All providers should review this report regularly to understand their current ASI position and track their progress over time. Find out more about this report.
There are two slot availability enquiries in e-RS which provide real-time information on used and unused slots by specialty, clinic type and priority over a specified time period. One is available to those with a service definer role within provider organisations and the other to those with a commissioner role, showing information for a specified provider.
For providers there are two reports on e-RS, which are available to those with an information analyst role. These show past slot utilisation (S6) and future slot utilisation (S7) at specialty and service level. In the future slot utilisation report, available slots, appointments booked via e-RS, and unused slots are displayed by priority and week, over a 26-week period. In the past slot utilisation report, available slots, appointments booked via e-RS, and unused slots are displayed by priority and week for the last thirteen weeks.
A new dashboard for providers has been published by the e-RS Programme which, among other measures, gives information about ASIs and their management.
Finally, users with the information analyst role who work for commissioners or providers can see detailed information on the management of all referrals, including ASIs, within the e-RS extracts. However, users will require high level analysis skills and experience of using the NHS e-Referral Service to interpret the data contained within the extracts
Future ASI improvements and support information
Future improvements on the ASI process will be updated on the e-RS news page.
Support information can be found within the e-RS system Help.
Last edited: 14 July 2025 11:41 am