The good news is that, over the past few years, a number of ‘shared care records’ have been developed across the country, including the Leeds Care Record, the Care and Health Information Exchange in Hampshire, Connecting Care in Bristol and the Oxford Care Record, where professionals can access record information from different sources, with this information usually displayed to them in different tabs.
These have provided benefit but, at the same time, have not operated to common standards.
So now we’ve also got a better understanding of how we best go about delivering information sharing projects. We know these need to be locally led, so that we can establish the local relationships with care professionals and patients, and to be delivered in a way that grows, develops and cultivates those relationships. We know that they need to focus on real-world problems for care professionals and service users, but also to establish and maintain trust in how information is shared and used so that we address information governance aspects upfront. As one of my NHS England colleagues said, “Trust takes a time and effort to build, but the work of a moment to break.” The point is fundamental to any information sharing initiative.
At the same time, and in light of the NHS Long-Term Plan, we now need to move beyond this basic ability to access information to be able to support a wider set of user needs, including proactive prevention and redesigning of local services through the use of data to enable clinical decision-support, identify gaps in care and drive insight.
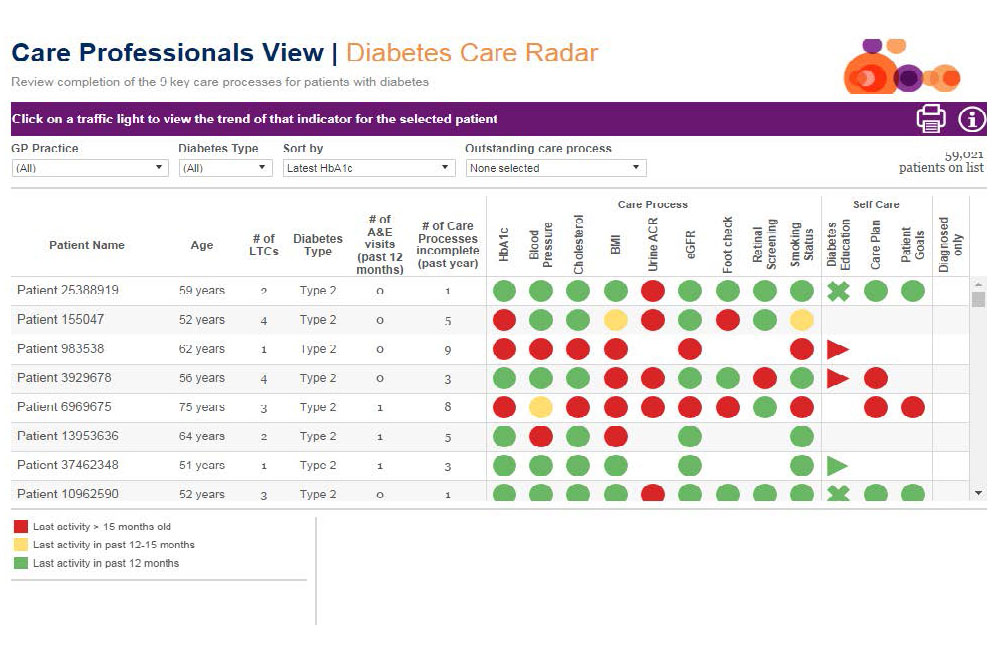
This will help to enable a shift in how services are provided, with an increasing focus on prevention of disease and disease progression and on enabling improvements in the health and wellbeing of a whole population. This should allow a better understanding of how our services impact people’s lives and how we can adopt an approach of continuous data-driven quality improvement. There are already some examples of this such as the Diabetes Radar in North West London, which identifies gaps in care along a diabetes pathway.
The Local Health and Care Record approach
To help learn from past experiences, we’ve developed the following principles to underpin the LHCR approach. They outline the insight that we have gained from previous initiatives, the evidence behind these and how this has helped formulate the LHCR approach. The first and foremost is that “maintaining trust is key". That means establishing trust but also maintaining it as we progress.
|
Insight
|
Evidence
|
Approach
|
|
Maintaining trust is key
|
Citizen juries. Concerns of Care.data
|
Local buy-in. Requires local projects to engage public and professionals
|
|
Driven by local service transformation
|
Aligns to the Long Term Plan direction
|
Delivery that is directly aligned to national and sustainability and transformation partnership (STP)/ integrated care system (ICS) priorities
|
|
Establish local ownership
|
60+ existing shared care records initiatives
|
Nationally co-ordinated and locally-led delivery. Based on sustainable footprints and population flows
|
|
Maximise the use of data
|
Establish a Learning Health System
|
Create longitudinal, normalised record to enable individual care, planning and other uses (such as research)
|
|
Standards-based, federated architecture
|
Open Banking
|
Promote standard-based interoperability with open platform principles and the use of common components
|
|
Build on learnings from the more advanced places
|
Wachter Review
|
Deliver in a series of waves of implementation
|
In line with the Wachter Review recommendations, we are starting with a number of areas that can we learn from. As a result, we have selected five areas to be Local Health and Care Record Exemplars (LHCREs), which will then assist and share learnings with other areas delivering Local Health and Care Records (LHCRs).
What does the public think?
As we start this journey, we need to make sure that we have engaged with the public on the sharing of their data and their control of its use. The principle must be that “Data is there for the asking, not taking”.
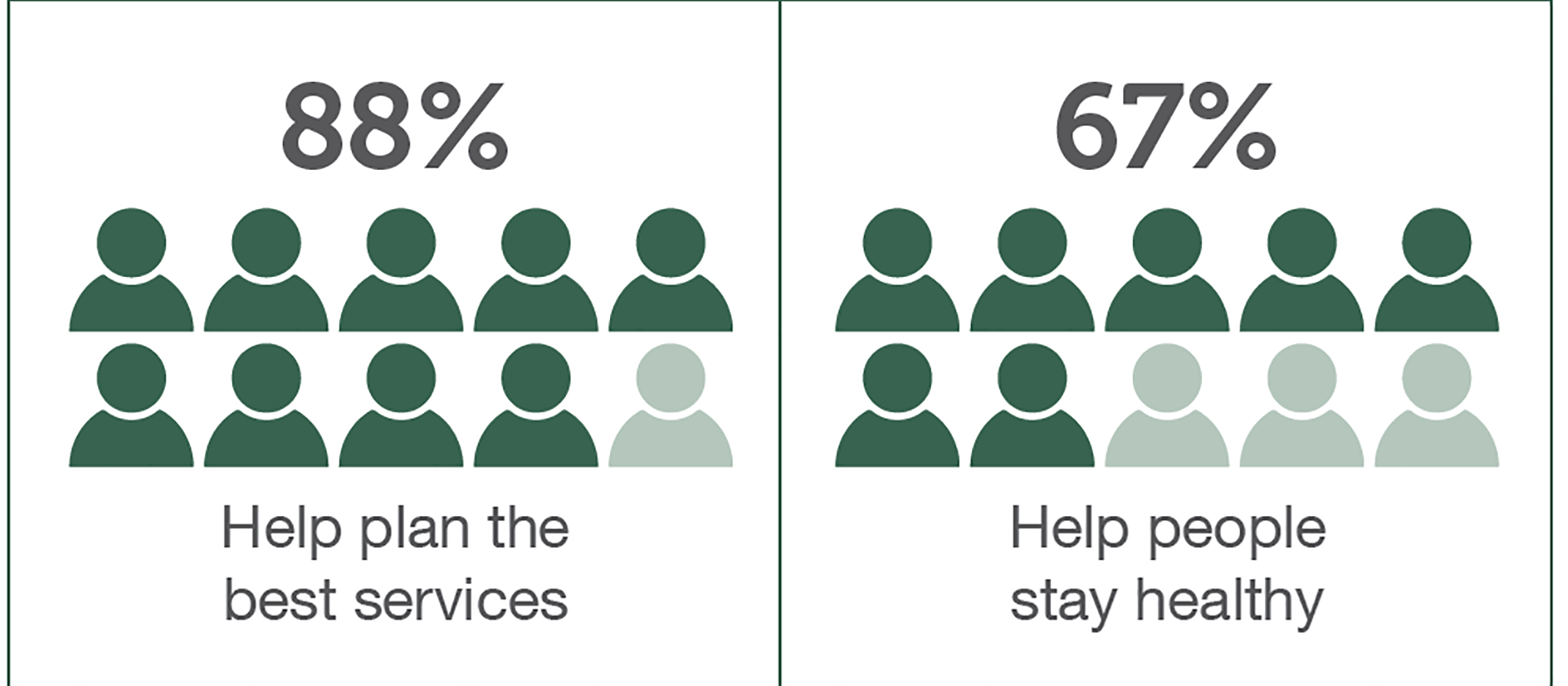
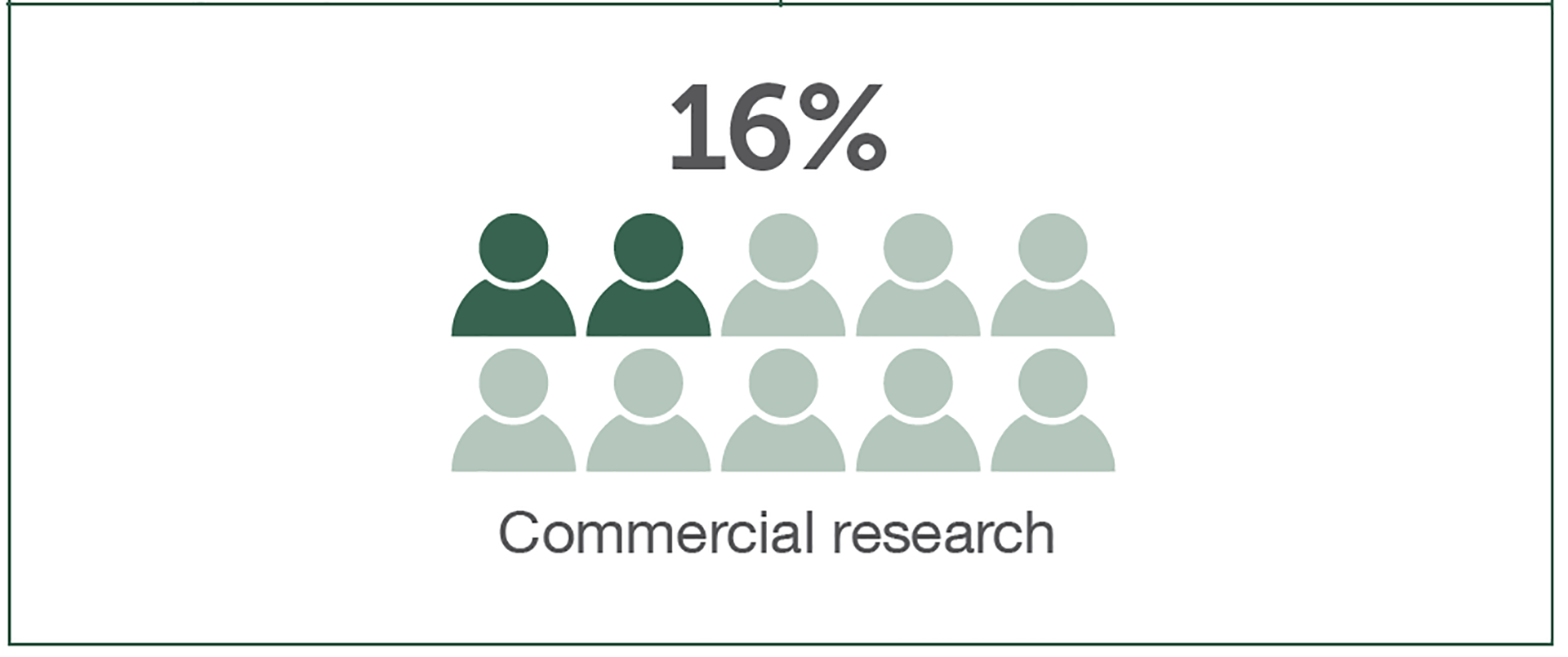
Several Local Health and Care Records Exemplars (LHCREs) have started their work with research on public expectations: specifically, how people wish to be engaged in the sharing and use of their data and what controls need to be in place. A good example is Yorkshire and Humber LHCRE‘s recent report on the members of the public they engaged with:
This has highlighted support for the use of information to help improve care outcomes, but, at the same time, the report outlines a number of concerns and challenges that we need to jointly work through.
“What should health and care information be used for?” (public responses to a Yorkshire and Humber Care Record survey)

What will Local Health and Care Records deliver?
Local Health and Care Records build on and move beyond the existing shared care records, which corralled information into different tabs, to a place, with LHCRs, where we can provide a single consolidated and standardised view from across the different venues of care (for example, viewing a consolidated set of medications) and delivered using open platform principles.
This is a significant step: taking data from multiple sources with varying levels of data quality, mapping this onto common patient identifiers, aligning with common terminologies, and standardising its representation. This provides a consistent representation for care professionals. It also provides feedback to source systems on improving data quality at source as they open up their systems through APIs.
This also enables an ecosystem of ‘apps’ able to draw on this data in a safe manner and with clear audit controls. Examples include the creation of care plans jointly developed and owned by individuals with the professionals caring for them and real-time algorithms to identify those at risk.
We know this is long journey but the approach must be to progress in iterations and take the learning to guide us. Our LHCRE communities are delivering in a iterative fashion, demonstrating functionality on priority pathways tied to local service transformation needs whilst ensuring that the information governance considerations are designed upfront. Each LHCRE has locally selected their priorities. Cancer in Yorkshire and Humber and Dementia and Frailty in Greater Manchester are examples of the approach. They are then ‘blueprinting’, so others don’t need to start from scratch.
In the first phase, LHCREs will be demonstrating that solutions are ‘usable, useful and used’, delivering the following functionality:
- a consolidated ‘longitudinal’ health and care record across venues of care to support care-co-ordination
- a consolidated de-identified ‘longitudinal’ health and care record across venues of care to support subsequent uses, such as population planning
- use of this data to enable joint care planning
- use of this data to enable a real-time algorithm for insight
- enabling patient access and contributions to the LHCR record through the NHS App
- providing an extract of data (for example, to enable national benchmarking)
- linking to genomic summary reports
And these LHCREs need to interoperate through Open APIs, so information can be accessed as patients move across geographic boundaries or organisations.
Co-production?
As part of the delivery, the LHCR programme is co-producing standards with the LHCREs that the exemplars need to implement as part of delivering the above functionality. These include:
- the ‘longitudinal’ care record definition being developed the Professional Records Standards Body on the content of the care record. They have already had over 250 attendees providing comments at their various sessions
- the Information Governance Framework for information sharing for the LHCRs, starting with the controls for individual care and then moving onto secondary uses. Journey 1 (individual care for a LHCRE) has already had over 400 comments. This framework being clear on the legal and transparency requirements placed on LHCRE
- the ‘Cyber Standard’ developed in conjunction with NHS Digital and the National Cyber Security Centre
- the ‘LHCR architecture capabilities’ that a LHCRE needs to deliver. These definitions being co-produced by LHCREs, NHS Digital and NHS England architects
- the interoperability standards including the FHIR Care Connect profiles and APIs that each LHCREs will expose that are being co-produced with INTEROpen and NHS Digital
We also have a number of LHCRE networks such as the care professional, social care and evaluation networks driving the delivery, as this is a care professional (not a technology) -led programme.
We are also working with NHS Digital colleagues on the delivery of common national components to be used across the LHCREs. These includes the National Record Locator, NHS Login, and the federated de-identification component, as well as iteration of national services to suit local needs.
It’s recognised that localities are at different places and that we need to get the right balance between ‘one size fits all’ and letting ‘a thousand flowers bloom,’ while keeping momentum in local delivery. LHCREs will produce a handful of ‘topologies’ that allow other LHCRs to identify which one they are closest to and, for those areas that have little already, they can then “leapfrog” some of the legacy considerations. It avoids us waiting for a perfect single model for all localities when we know one size will not cater for all the different starting points . As a example, we have five LHCREs with different technical topologies.
- GM – a single instance of a shared care record, with a standardised and consolidated care record data layer being established that integrates with this.
- TVS – a standardised and consolidated care record data layer that integrates with the many different shared care records.
- Wessex – a standardised and consolidated care record data layer developed by linking two shared care records.
- OneLondon – a standardised and consolidated care record from multiple interoperating data layers sitting on top over a set of health information exchanges.
- Yorkshire and Humber – a federated model to access data, which then forms a standardised and consolidated data layer for individual care and population health.
Who are they?
The first five Local Health and Care Record Exemplars cover over 40% of the population and were selected purposely to cover urban-rural and demographic variance. Subsequent LHCRs are being mobilised to be part of Wave 2.

We are already seeing early progress being made, such as the proactive identification of patients that are potentially frail in OneLondon and accessing of results and referrals in Wessex. In subsequent blogs, we will look at these more closely.
We will also be running a set of ‘Learning from local‘ events in the near future to share learning. For more details, please register with NHS Futures Learning from Local or contact [email protected]
Finally, I want to thank and acknowledge those who have helped formulate the approach, provided ideas and outlined the challenges that we need to work through on this journey, including Matthew, John, Simon, Will, Luke, Lisa, Stephen, Hadley, Terence, Julie, Richard, Joe, Ewan, Phil, Sam, Dawn, Rachel, Katie, Tom, Sarah and many, many others…




